点击上方国际母乳会LLL 设为星标,获取哺乳信息
你是否在母乳喂养时感到疼痛,可能还伴随着宝宝体重增长缓慢?虽然绝大多数这种哺乳问题可以通过调整哺乳和含乳姿势,再加上良好的母乳喂养管理来解决,但有时候舌系带过紧可能也会造成哺乳问题。


识别舌系带过紧


母乳喂养会受到怎样的影响
宝宝可能:
根本无法含住乳房 不能较深地含乳,导致乳头疼痛和损伤 难以持续含住乳房,发出“咔哒”声像是吸不住乳房 应对快速流动的乳汁时,会噗噗地呼气和呛奶 需要频繁哺乳才能吃到足够的奶量 体重增长不佳,或需要补充奶来保持足够的体重增加 出现需要治疗的黄疸 当乳汁流速减慢时,在乳房上很烦躁 出现肠绞痛
妈妈可能会经历:
哺乳时疼痛,伴有乳头损伤。刚喂完奶乳头可能被压扁或变形成楔形,就像新口红的形状一样,往往乳头尖上有一条横纹。 由于无效的乳汁移出而导致乳房肿胀、乳管堵塞和乳腺炎。 由于无效的乳汁移出而导致产奶量低 奶量过多——如果宝宝通过频繁吃奶来弥补哺乳不足的话 感到疲劳、沮丧和挫败 过早停止母乳喂养
母乳喂养对每个宝宝都很重要
治疗
继续母乳喂养
软化乳房
生物养育法™

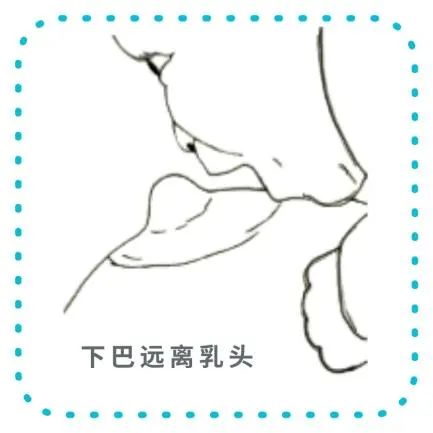
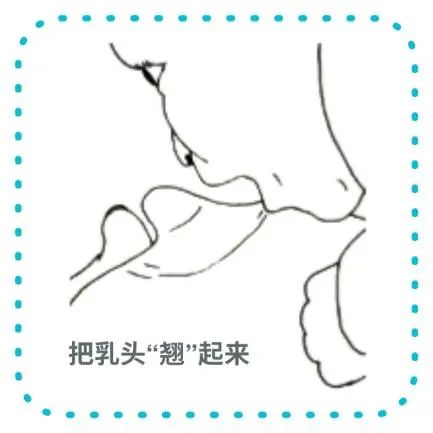
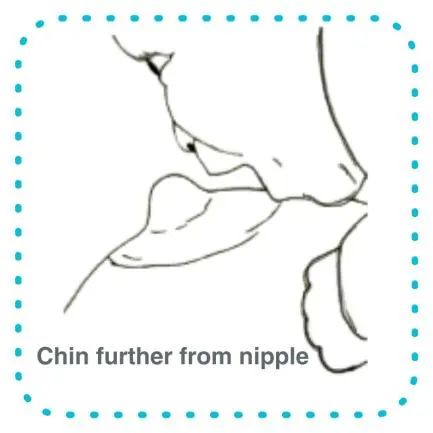
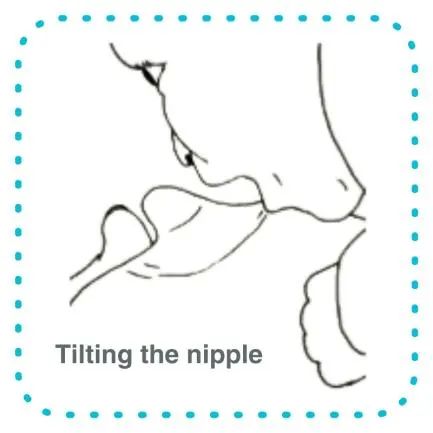
较深地含乳
鼓励舌头的活动
为了鼓励宝宝把舌头往前伸,你也可以尝试:
你半躺着,让宝宝趴在你身上。你试着往前和往后调整自己身体的角度,来感受重力作用是如何影响舌头位置的。 鼓励宝宝在喂奶前后舔自己嘴唇或你的乳头上的乳汁。 你向宝宝伸出自己的舌头,来鼓励他模仿你。
维持住奶量
上腭异常
以下方法会有所帮助:
先把指甲修剪整齐,并洗干净手指
触摸宝宝的嘴唇,等到他们张开嘴
轻轻滑入你的手指,指腹朝上沿着他的硬腭伸入,触发呕吐反射前停下。
治疗舌系带过紧
能做什么?
舌系带松解术 ——把舌系带松解开——可以极大地提高妈妈和宝宝母乳喂养的舒适度和效率。松解开舌系带是一个又快又简单的手术。六个月以下的宝宝不需要麻醉。
等待是一种选择吗?
有时候很薄的舌系带会自然断开,或者可以通过轻柔按摩舌系带被拉伸开。舌系带越早松解开,母乳喂养的困难就越容易解决。为六个月以上的宝宝松解舌系带是一个比较复杂的手术,通常需要全身麻醉。
舌系带松解术 ——会怎么做?
在医生初步评估后,宝宝会被包裹起来抱着(通常由助手抱着) ,所以在手术中他会保持不动,只需要一两分钟即可。医疗人员抬起宝宝的舌头,用一把圆头的无菌剪刀或高温烧灼消毒的剪刀,把舌系带松解开。
这个手术疼吗?
如果问题没有解决?
通常妈妈注意到哺乳时她的舒适感会立刻改善。有时宝宝需要一到两周来适应舌头变得更灵活了。大一点的宝宝会发现较难适应舌头增加的灵活性,就会建议给他们进行舌头锻炼。偶尔宝宝的舌系带需要第二次松解,通常是因为第一次松解得不够彻底。如果你怀疑最初的手术没有解决宝宝的母乳喂养问题,就要另行咨询。要坚持去寻找解决方案。如果涉及好几个因素,解决问题就需要时间和专业知识。国际母乳会的哺乳辅导可以建议更多的探索方式,并提供持续的支持。
乳头疼痛
湿敷伤口愈合法
乳头皲裂处的血
如果愈合缓慢
寻求帮助
2022-09-03


你可以在此找到离你最近的哺乳辅导。
A baby may:
Be unable to latch on to the breast at all. Be unable to latch on deeply, causing nipple pain and damage. Have difficulties staying on the breast, making a clicking sound as he loses suction. Splutter and choke when coping with fast flowing milk. Breastfeed constantly to get enough milk. Have poor weight gain or need supplementation to maintain adequate weight gain. Develop jaundice that needs treating. Be fussy at the breast when the milk flow slows. Develop colic.
A mother may experience:
Pain during feeds, with damaged nipples. Her nipple may be compressed or distorted into a wedge shape like that of a new lipstick immediately after feeding, often with a stripe at its tip. Engorgement, blocked ducts and mastitis because of ineffective milk removal. Low milk production because of ineffective milk removal. Oversupply—if her baby compensates for not being able to breastfeed well by nursing very frequently. Tiredness, frustration and discouragement. A premature end to breastfeeding.
Keeping breastfeeding going
Soften your breast
A baby often instinctively attaches more deeply and comfortably if they can snuggle up close to their mother’s chest for periods of time. Try letting your baby lie on your body as you recline so both their chest and tummy are against you. This kind of ‘laid-back’ breastfeeding contact is known as Biological Nurturing™ and can be done skin-to-skin or with you and your baby lightly clothed—whatever is more comfortable and convenient for you both. Because gravity helps a baby keep their tongue forwards, this can make a real difference to how well your baby feeds and how much milk you make.

Help your baby get as deep a latch as possible at the breast. This will maximize the amount of milk they get and minimize nipple pain.
Encourage tongue mobility
• Reclining with your baby on top of you. Try leaning forward and back yourself to understand how gravity affects tongue position.
• Encouraging them to lick milk from their lips or from your nipple before and after feeds.1-9
• Sticking your tongue out at your baby to encourage them to copy you.
Maintain milk production
An unusual palate
The following may help.
• Touch your baby’s lips and wait until they open their mouth.
• Gently slide in your finger, pad side up along his hard palate, stopping just before the gag reflex is triggered.
Treating Tongue Tie
Frenotomy—dividing the tongue tie—can dramatically improve breastfeeding comfort and efficiency for both mother and baby. Dividing a tongue tie is a quick and simple procedure. No anaesthetic is needed for a baby under six months of age.
Sometimes a very thin tongue tie breaks spontaneously or can be stretched by gentle massage of the frenulum. The earlier a tongue tie is divided, the easier it is to resolve any breastfeeding difficulties. Dividing a tongue tie in a baby over six months old is also a more complicated procedure and usually requires a general anaesthetic.
After the health professional’s initial assessment, your baby will be swaddled and held (often by an assistant) so they stay still during the procedure, which only takes a minute or two. The health professional lifts the tongue and divides the frenulum by cutting it with a pair of round-ended sterile scissors or by cauterising it.
No anaesthetic is needed for a very young baby as having a tongue tie divided only hurts a little, if at all. Some babies protest more at being swaddled than about the treatment. Others sleep right through the procedure! You will be asked to breastfeed your baby as soon as the procedure is over, to offer comfort, clean the wound and get their tongue moving as soon as possible. The inside of a baby’s mouth heals very quickly. The only treatment usually needed is to breastfeed to keep the wound clean and keep his tongue mobile. There may be a white patch under your baby’s tongue, but this heals within 24 to 48 hours.
Usually a mother notices an instant improvement in her comfort during breastfeeds. Sometimes it takes a week or two for a baby to adjust to their tongue’s greater mobility. An older baby may find it harder to adjust to increased tongue mobility and tongue exercises may be recommended. Occasionally a baby’s frenulum needs dividing a second time, usually because the division was not quite extensive enough the first time. If you suspect that the initial procedure has not resolved your baby’s breastfeeding problems arrange another consultation. Do persist with finding solutions. If several factors are involved it can take time and expertise to resolve the problem. An LLL Leader can suggest further paths to explore and provide ongoing support.
Blood from cracked nipples
If healing is slow
参考文献 References
Hazelbaker, AK. Tongue-Tie: Morphogenesis, Impact, Assessment and Treatment. Columbus, OH: Aidan and Eva Press, 2010.
Mohrbacher, N. Breastfeeding Answers Made Simple. Amarillo Tx: Hale Publishing, 2010.
Watson Genna, C. Supporting Sucking Skills in Breastfeeding Infants. Burlington, MA. Jones & Bartlett, 2012.
Geddes, DT. et al. Frenulotomy for breastfeeding infants with ankyloglossia: Effect on milk removal and sucking mechanism as imaged by ultrasound. Pediatrics 2008; 12(1):e188–94.
Hogan, M. Westcott, C. and Griffiths, M. Randomized, controlled trial of division of tongue-tie in infants with feeding problems. J Paediatr Child Health 2005; 41:246–50.
Hong, P. et al. Defining ankyloglossia: A case series of anterior and posterior tongue ties. Int J Ped Otorhinolaryngology 2010; 74:1003–6.
Knox, I. Tongue tie and frenotomy in the breastfeeding newborn. Neoreviews 11 (9) Sept 2010.
Miranda, BH. and Milroy, CJ. A quick snip—a study of the impact of outpatient tongue tie release on neonatal growth and breastfeeding. JPRAS 2010; 63:e683–5.
NICE Guidelines
Watson Genna, C. And Coryllos, EV. Breastfeeding and tongue-tie. J Hum Lact 2009; 25(1):111–2.
资料来源:https://www.laleche.org.uk/tongue-tie/

END
作者:英国母乳会
翻译:传艳
审稿:Lynn、Marien、张艳莹、核桃

找到我们
微信公众号|视频号|小红书|抖音|新浪微博|今日头条|哔哩哔哩|优酷
搜索关键字“国际母乳会LLL”


更多阅读资料,
欢迎大家访问“国际母乳会LLL”官网:
https://www.muruhui.org/
分享
收藏
点赞
在看
正如我们的志愿者在内部会议中提到,投身公益事业后才知道做公益也是有成本的!你的支持和赞赏可以让更多的妈妈获益!
本篇文章来源于微信公众号: 国际母乳会LLL